By Jorge C. Coro, DMD, MS, and Ivette M. Coro, DMD
 Figure 1. Top, example of a Multi-Loop Edgewise Archwire (MEAW). Bottom, examples of activations of the MEAW.Early in the 1970s, Young H. Kim, DDS, DMD, MS, developed the Multi-Loop Edgewise Archwire (MEAW) appliance in his Weston, Mass, practice. This appliance allowed him to treat open bites and other severe malocclusions with excellent clinical results.1
Figure 1. Top, example of a Multi-Loop Edgewise Archwire (MEAW). Bottom, examples of activations of the MEAW.Early in the 1970s, Young H. Kim, DDS, DMD, MS, developed the Multi-Loop Edgewise Archwire (MEAW) appliance in his Weston, Mass, practice. This appliance allowed him to treat open bites and other severe malocclusions with excellent clinical results.1
Meanwhile, in the Department of Orthodontics at Kanagawa Dental College, Sadao Sato, DDS, DDSc, was investigating the etiology of different malocclusions and concluded that the posterior occlusal plane was the primary determinant of mandibular position. However, Sato could not find an appliance that would control the occlusal plane in the manner he wanted. When he attended a course in 1985 given by Kim in Tokyo, he realized that with the MEAW appliance he could apply his principles of occlusal plane control to influence mandibular position. Sato and his colleagues developed mechanics with the MEAW appliance in which they were able to efficiently treat even the most severe malocclusions by controlling the maxillary occlusal plane in three dimensions.2
 Figure 2. Facial and intraoral photos of a 26-year-old female patient.
Figure 2. Facial and intraoral photos of a 26-year-old female patient.
MEAW–The Ultimate Functional Appliance
Unlike most other functional appliances that disarticulate the dentition in an attempt to modify the skeletal framework, the MEAW appliance uses the action of opposing cusps and fossae and their proprioceptive input to guide mandibular position. The individual teeth act as integral members that make up the occlusal plane.
The MEAW appliance is made from .016 x .022 Blue Elgiloy, which is supplied in 14-inch lengths. One MEAW incorporates most of that 14-inch length, which is indicative of its flexibility. Kim conducted studies that demonstrated a very low load-deflection rate of the MEAW wire when compared to straight stainless steel archwires (Figure 1).3
The main component of the MEAW is the boot loops, which begin distal to the maxillary and mandibular lateral incisors and continue at each of the interproximal contact areas of the buccal segments. The loops represent almost an inch of interbracket wire length that acts to dissipate the forces from tooth to tooth.4
 Figure 3. Pretreatment cephalometric radiograph of the patient.The loops provide effective three-dimensional control of the individual teeth that work in concert to control the occlusal plane(s). The basic activation of the MEAW is progressive tip back, which when used in conjunction with anterior vertical elastics, acts to distally upright and intrude the molars and bicuspids while controlling incisor extrusion (Figure 1). This steepens the maxillary occlusal plane and flattens the mandibular occlusal plane. This action in open bite cases allows for counterclockwise adaptation of the mandible to close the bite.
Figure 3. Pretreatment cephalometric radiograph of the patient.The loops provide effective three-dimensional control of the individual teeth that work in concert to control the occlusal plane(s). The basic activation of the MEAW is progressive tip back, which when used in conjunction with anterior vertical elastics, acts to distally upright and intrude the molars and bicuspids while controlling incisor extrusion (Figure 1). This steepens the maxillary occlusal plane and flattens the mandibular occlusal plane. This action in open bite cases allows for counterclockwise adaptation of the mandible to close the bite.
Other activations of the appliance include stepping the loops up or down. By doing so, the three-dimensional orientation of the occlusal planes and the vertical dimension can be readily controlled. The main vertical activation is placed on the second loop (distal to the canines) and is particularly effective in leveling the deep Curve of Spee typically seen in deep bites and Class II malocclusions. The wires need to be removed to place activations every 4 weeks for maximum efficiency.4
Elastics provide the forces that complement the archwire activations. Anterior vertical elastics allow the tip back activations to express their action, while short Class II and Class III elastics provide the anterior or posterior component of force. These antero-posterior vectors need to be kept short in order to avoid the unwanted effects that longer antero-posterior intermaxillary forces have on the occlusal plane.4
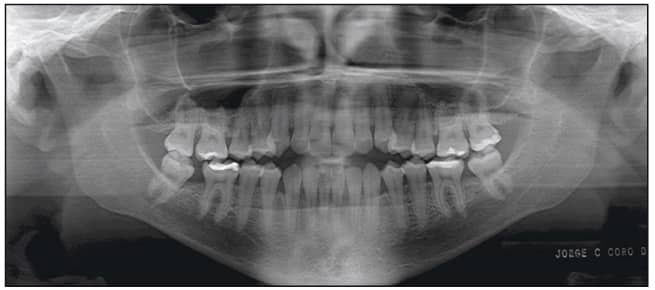 Figure 4. Pretreatment panoramic radiograph of the patient.The vertical component of force afforded by these configurations of elastics augment the lack of muscle tonicity of the perioral musculature of patients with these types of severe malocclusions. The elastics commonly used are 6 ounce, 3/16 inch.4
Figure 4. Pretreatment panoramic radiograph of the patient.The vertical component of force afforded by these configurations of elastics augment the lack of muscle tonicity of the perioral musculature of patients with these types of severe malocclusions. The elastics commonly used are 6 ounce, 3/16 inch.4
High Angle Class III Malocclusion
High angle Class III and Class I open bite malocclusions tend to exhibit flexion of the cranial base.5 This flexion produces a deficient antero-posterior dimension of the maxilla which causes posterior dento-alveolar discrepancy. The developing molars do not have sufficient space and are essentially “squeezed out,” resulting in excessive vertical development of the posterior maxilla. This in turn causes a flattening (downward direction in the posterior) of the occlusal plane. The mandible adapts to the increased vertical height of the molars through anterior rotation, resulting in a protrusive displacement. In cases where there is weak perioral musculature, such as in mouth breathers, the mandible cannot adapt anteriorly and tends to rotate down and back, resulting in an open bite.6 By alleviating the posterior discrepancy and “reconstructing” the occlusal plane (tipping it down in front), Class III cases can be treated with excellent, stable results.4 Figure 5 (left). Day of placement of the MEAW appliance. Figure 6 (right). Eight weeks after placement of the MEAW appliance.
Figure 5 (left). Day of placement of the MEAW appliance. Figure 6 (right). Eight weeks after placement of the MEAW appliance.
High Angle Class III Case Report
The patient, a 26-year-old female, presented with a chief complaint that she did not like her smile and was unable to bite with her front teeth. She presented with a concave profile due to an apparent midface deficiency and mandibular prognathism. She had a Class III anterior open bite malocclusion, confirmed by the cephalometric analysis (Figures 2 to 4).
The posterior discrepancy was eliminated by extraction of the existing three third molars. Leveling and aligning took 6 months with the use of .014 and .016 Sentalloy archwires. Interferences to mandibular adaptation were eliminated by creating a posterior open bite. Mandibular adaptation occurred within 8 weeks as the anterior open bite closed and a Class I relationship was established (Figures 5 and 6).
 Figure 7. Facial and intraoral photos of the patient on debond day.
Figure 7. Facial and intraoral photos of the patient on debond day.
During the next 8 months of treatment, the occlusal plane was successfully reconstructed (tipped down in the front and steepened). Detailing ensured a stable functional occlusion. The patient was debonded and instructed to indefinitely wear an upper and lower thermoformed retainer a minimum of three nights per week (Figures 7 to 12).
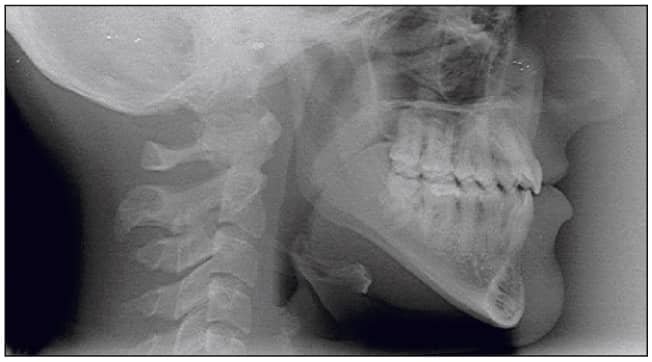 Figure 8. Post-treatment cephalometric radiograph.
Figure 8. Post-treatment cephalometric radiograph.
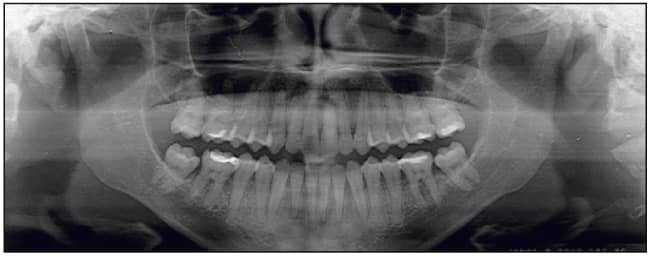 Figure 9. Post-treatment panoramic radiograph.
Figure 9. Post-treatment panoramic radiograph.
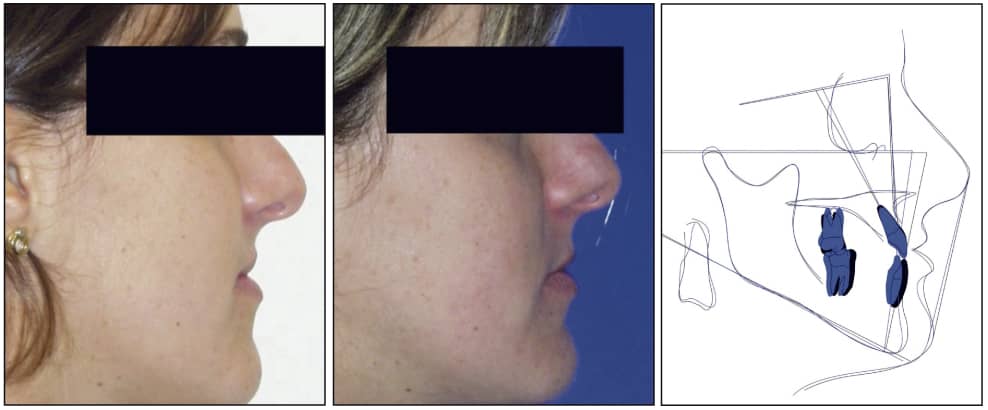 Figure 10 (left and center). Comparison of patient’s profile pre- and post-treatment. Figure 11 (right). Pre- and post-treatment superimposition.
Figure 10 (left and center). Comparison of patient’s profile pre- and post-treatment. Figure 11 (right). Pre- and post-treatment superimposition.
 Figure 12. Comparison of patient’s smile pre- and post-treatment.
Figure 12. Comparison of patient’s smile pre- and post-treatment.
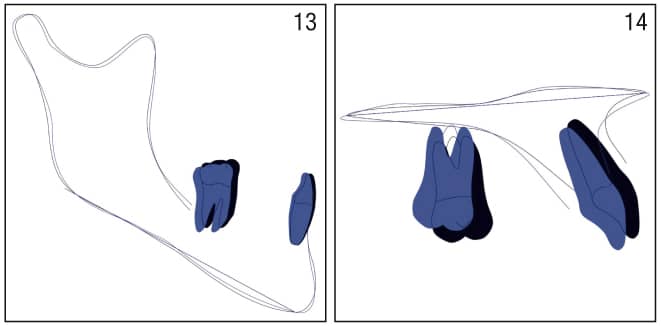 Figure 13 (left). Mandibular superimposition at corpus- menton. Figure 14 (right). Maxillary superimposition at palatal plane.
Figure 13 (left). Mandibular superimposition at corpus- menton. Figure 14 (right). Maxillary superimposition at palatal plane.
GUM Metal
Treatment with MEAW continues to evolve. A new superelastic titanium alloy developed by Toyota Central R & D Laboratories has made its way into orthodontics in Japan, as Tokyo-based Rocky Mountain Morita Corporation introduced GUM Metal archwires to that market. This new alloy exhibits the elastic properties of NiTi, yet can be bent as readily as Blue Elgiloy wires. Pioneers like Akiyosi Shirazu, DDS, DMedSci, have incorporated these wires into their MEAW treatment with great early results. Due to the unique properties of this new alloy, smaller vertical or omega loops replace the boot loops, which provides very effective force levels and much greater patient comfort. RMO will be introducing these wires to the US market in the coming year. OP
Jorge C. Coro, DMD, MS, is in private practice in Coral Gables, Fla. He teaches the MEAW course in the graduate orthodontic programs at Nova Southeastern University and the University of Florida. He can be reached at [email protected].
Ivette M. Coro, DMD, is an orthodontic resident at Nova Southeastern University. She can be reached at [email protected].
References
1. Kim YH, Han UK, Lim DD, Serraon ML. Stability of anterior openbite correction with multiloop edgewise archwire therapy:A cephalometric follow-up study. Am J Orthod Dentofacial Orthop. 2000 Jul; 118(1):43-54.
2. Fushima K, Kitamura Y, Mita H, Sato S, Suzuki Y, Kim YH. Significance of the cant of the posterior occlusal plane in class II division 1 malocclusions. Eur J Orthod. 1996 Feb; 18(1):27-40.
3. Yang WS, Kim BH, Kim YH. A study of the regional load deflection rate of multiloop edgewise arch wire. Angle Orthod. 2001 Apr; 71(2):103-9.
4. Sato S, Akimoto S, Matsumato A, Shirasu A, Yoshida J. Chapter Five MEAW Manual. Kanagawa Dental College, Orthodontic Department Autumn 2001.
5. Hopkin GB, Houston WJ, James GA. The cranial base as an aetiological factor in malocclusion. Angle Orthod. 1968 Jul; 38(3):250-5.
6. Sato S, Endo N, Yamauchi M, Takeuchi M, Suzuki Y. Importance of posterior discrepancy in the development of skeletal Class III malocclusion. Kanagawa Shigaku. 1989 Jun; 24(1):219-29.