By Robert Miller, DMD
By Robert Miller, DMD
A recent study published in the American Journal of Orthodontics and Dentofacial Orthopedics found that the correction of Class II malocclusion cases is primarily a result of the stable interdigitation of the posterior teeth. The findings, the result of a 32-year follow-up study conducted by Pancherz et al, also noted a number of factors in relapse for these cases, including bad oral habits and poor retainer compliance.1 With over 53% of orthodontic patients having a mild to moderate Class II malocclusion,2 orthodontists have been exploring new innovative options to accelerate treatment for these types of patients and avoid the risk of relapse.
Although many of our patients come to us looking to correct a Class II malocclusion, most choose not to go through surgery. In treating these nonsurgical patients, I have found a number of new technologies that contribute to faster, more effective treatment overall. I have found success using a combination of treatment innovations, including the Xbow™ Class II Corrector, Esprit™ springs from Opal Orthodontics, and AcceleDent® from OrthoAccel® Technologies Inc.
[sidebar float=”right” width=”250″]Introducing an Accelerated Option: A Treatment Coordinator’s Perspective
By Sarah Keller
One evening I was asked to research AcceleDent®, from OrthoAccel® Technologies Inc, to see if it could be something our patients would want. As soon as I finished reading about the SoftPulse Technology® and how this device works to stimulate gentle, healthy tooth movement, I looked up from my computer screen and shouted, “Who WOULDN’T want this?!”
Studies show that:
- A majority of patients feel that orthodontic treatment takes too long.1
- 96% of consumers consider reduction in discomfort as an important benefit with orthodontic treatment.2
- 7 out of 10 patients are not offered an accelerated treatment option.2
I could think of a handful of patients who would immediately jump at the opportunity to accelerate their treatment. After ordering our AcceleDent units, I sent an email to every past, present, and future patient in our database letting them know that an accelerated treatment option was available to them. Our patients’ response was just as I predicted: All of the units ordered were presold, and we placed a second order within days.
A device like AcceleDent provides practices an opportunity to address patient complaints about treatment time and discomfort without having to compromise on the quality of treatment. But patients aren’t the only ones who benefit when a new technology like this is introduced. Practices that offer accelerated treatment options are able to differentiate themselves from other practices in the market and increase patient compliance with various treatment modalities, which goes a long way to improving practice efficiency and profitability. OP
Sarah Keller is an orthodontic treatment coordinator and office marketing coordinator based in the Houston area. As an orthodontic consultant, Keller coaches practices on how to increase case acceptance and patient satisfaction by effectively communicating the value of technology to patients.
[/sidebar]
The Xbow and the Esprit springs allow me to achieve what is traditionally the desired goal in orthodontics: to apply the most efficient force mechanics while avoiding root resorption. With the introduction of AcceleDent, we’re taking the process one step further—and faster. With it, we have come to understand that it’s not just about the efficiency of the force, but also the frequency of that force that makes a difference.
Modulation of Bone with Pulsatile Forces
I’ve been impressed with my clinical results when using AcceleDent, which applies cyclic forces to increase the rate of tooth movement. AcceleDent is an FDA-cleared Class II medical device that has been proven to speed up treatment by as much as 50%.3 The device delivers a light pulsatile force of 20 grams, which is significantly less than that of chewing.
While this technology is relatively new to orthodontics, the mechanical modulation of bone architecture that AcceleDent employs has been studied since the mid 1980s on skeletal diseases and problems such as fracture healing, osteoporosis, and other developmental deformities.4 Studies using pulsatile forces have demonstrated the increased rates of fracture healing and enhanced bone density in long bones.5,6 In fact, there’s an interesting dichotomy when comparing the structural and metabolic bone responsibilities.
Compare, for example, the cortical bone thickness of an elite tennis player with that of an astronaut who is in space for an extended period of time. The racquet side humerus of the tennis player is 25% to 30% thicker than the serving side. The astronaut has less structural demands, so metabolic function prevails and cortical thinning occurs. Furthermore, with regard to pulsatile forces, in animal studies that analyzed the effect of these forces in alveolar bone remodeling and tooth movement, remodeling occurred up to two and a half times faster with pulsatile forces and showed no increase in root resorption.7,8
AcceleDent in Action
AcceleDent is prescribed to a patient by an orthodontist, and the patient must comply by gently biting down on the device’s mouthpiece for 20 minutes daily during treatment. I have had no issues with patients complying with the regimen because they say it’s simple, easy to use, and can be used during low-maintenance activities such as reading or watching TV. What we hear most from patients is that they like AcceleDent and have no issues with compliance because of the device’s ability to reduce pain and discomfort. What I have learned over the course of treating the patients discussed below is that AcceleDent can be used with any fixed orthodontic appliance, and in conjunction with TADs, miniplates, or Class II springs.
To see what I’m talking about, let’s look at my recent Class II malocclusion patients who I treated using various combinations of the innovations mentioned above, plus AcceleDent.
Case 1
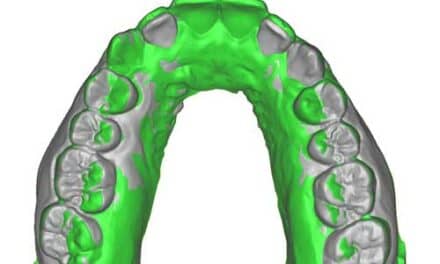
For one of my 14-year-old female patients, I needed to stabilize a Class I occlusion characterized by interdigitation of the first premolars (Figure 1A-E). When I ask orthodontists to predict how long they think this would take, they typically say around 24 to 30 months, but I was able to treat her in 16 months by using fixed appliances along with AcceleDent and the Xbow (Figure 1F-J). I decided to use both a noninvasive technique—AcceleDent—and an invasive technique—alveocentesis—to get the best results as fast as possible. Her severely displaced right second premolar benefitted from the alveocentesis.

Figure 1. (A-E) 14-year-old female patient with a Class I occlusion, characterized by interdigitation of the first premolars. (F-J) Patient treated in 16 months using fixed appliances as well as AcceleDent and the Xbow.
Case 2
There are, on occasion, adult patients who do not want orthognathic surgery and prefer to not have teeth removed. In this patient case study, the patient had an advanced maxilla (Figure 2A-C), so we used Bollard miniplates and Hugo De Clerck-type mechanics for the correction of the Class II discrepancy. She used AcceleDent for 20 minutes a day for all except 1 month of active treatment. I also used a horizontal vector on her for distalization, and after 6 months of using the AcceleDent we started to see distalization and space developing around the premolars and canines (Figure 2D-E).
At 11 months, the patient reported that her bite felt better and that she experienced minimal to no pain and discomfort as a result of using AcceleDent. She also added that reduction in pain served as a motivator to use her AcceleDent daily.
After 11 months, I removed her miniplates and started white Class II elastics. At 13 months, we were still resolving rotations on the patient’s left side in the mandibular arch. While I originally projected her treatment time would last 24 to 30 months, her total treatment time was actually 18 months. When looking at Figure 2, notice that her superimpositions show molar distalization and mandibular protrusion due to the crowding. However, we also were able to maintain torque in the maxillary arch and the maxillary incisors (Figure 2F-H).

Figure 2. (A-C) Patient presents with an advanced maxilla. (D-E) Shown at 6 months, distalization and space developing around the premolars and canines. (F-H) Patient completes treatment at 18 months.
Case 3
Here, another patient presents with a Class II open bite (Figure 3A-C). I recommended and performed a gingival graft in the anterior lower teeth. The patient had a habitual forward posture that resulted in a severe Class II malocclusion. Since this patient declined surgery, I retracted the maxillary segment of teeth 4 mm by limiting bite opening and maintaining torque. I also used TADs and AcceleDent in combination with fixed edgewise appliances.
This patient happened to be a smoker, so we began AcceleDent the same day that we placed the TADs, and waited 6 months (which was 6 weeks before loading). The TADs were placed in the infrazygomatic ridge (Figure 3D).
At the 6-month interval, the patient’s bite was slightly opening, so I added occlusal bite binders to her maxillary first molars. At the 9-month mark, the occlusal bite bonders were combined with 200 grams of force applied at or near the center of resistance. I finished the elastics with light vertical loading of the TADs at the 11-month mark. I originally projected that her treatment would have taken 24 to 30 months, but her actual treatment with AcceleDent was accelerated to 15 months (Figure 3E-G). Although she was a smoker, she reported minimal discomfort because of AcceleDent.

Figure 3. (A-C) Patient presents with Class II open bite. (D) TADs placed at 6 months in the infrazygomatic ridge. (E-G) Treatment completed at 15 months.
Case 4
This patient had a severe Class II malocclusion (Figure 4A-C), and we achieved good results with Xbow/Esprit in combination with AcceleDent using fixed edgewise appliances. Cephalometrically, she had incisor protrusion and maxillary protrusion but had a nice chin button. During Xbow therapy, she used AcceleDent for 20 minutes every day. After compensatory maxillary expansion, Esprit springs were added to the Xbow (Figure 4D-F). We overcorrected to half cusp Class III relationship of the first premolars.
At the 6-month point, I noticed that the spring was left at a half cusp Class III on the side that overcorrected, but I left the spring on the right side because it wasn’t as overcorrected as it was on the left. I removed all of the springs at the 7-month point, allowing the patient time to rebound. At the 8-month appointment, we affixed brackets using a precision indirect technique.

Figure 4. (A-C) Patient presents with Class II malocclusion. (D-F) Esprit springs added to the Xbow at 6 weeks. (G-I) Patient following treatment with Xbow and Esprit for 5 months, Avex MX for 9 months, and AcceleDent.
Note that the first month after the Esprit springs are removed is the point at which most rebounding occurs. At this point, the patient was a slight Class I with a slight Class II canine.
After 1 year, some rotations were still present, but rebound was complete and she was a Class II on both sides. Her total treatment time took 16 months, which is less than the original 24 to 30 months I projected (Figure 4G-I).
This case is particularly noteworthy because I used that combination of the new technologies I mentioned earlier—the Xbow, Esprit Class II Corrector, and AcceleDent. Additionally, we used the new Avex MX® bracket system from Opal Orthodontics to create a precision slot. Avex micro-milled brackets use precision bracket placement. This combination of manufacturing and placement precision resulted in unusually fast alignment. Growth in a favorable direction was the key to success in this case. However, the various innovative treatment modalities that we were able to use also contributed to the overall treatment success for this patient.
Conclusion
Orthodontists have several challenges when treating Class II malocclusion, including compliance, cooperation, resistance to surgery and/or extractions, root resorption, decalcification, pain, and discomfort. I’ve found that all of these challenges have the potential to be reduced when treating patients with AcceleDent. OP
 Robert Miller, DMD, a pioneer in the area of orthopedic correctors, lectures on precision bracket placement, temporary anchorage devices (TADs), Class II correctors, and treatment protocols for unique orthodontic appliances. Miller earned his DMD from The Medical University of South Carolina and completed his orthodontic residency at the Medical College of Virginia. He served for 3 years in the USAF as Chief of Orthodontics at Clark Air Base in the Philippines. He is past president of the Virginia Association of Orthodontics.
Robert Miller, DMD, a pioneer in the area of orthopedic correctors, lectures on precision bracket placement, temporary anchorage devices (TADs), Class II correctors, and treatment protocols for unique orthodontic appliances. Miller earned his DMD from The Medical University of South Carolina and completed his orthodontic residency at the Medical College of Virginia. He served for 3 years in the USAF as Chief of Orthodontics at Clark Air Base in the Philippines. He is past president of the Virginia Association of Orthodontics.
REFERENCES
Miller
- Pancherz H, Bjerklin K, Lindskog-Stokland B, et al. Thirty-two-year follow-up study of Herbst therapy: A biometric dental cast analysis. Am J Orthod Dentofacial Orthop. 2014;145:15-27.
- Proffit WR, Fields HW, Moray LJ. Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the NHANES-III survey. Int J Adult Orthod Orthogn Surg. 1998;13:97-106.
- Data on file. OrthoAccel Technologies Inc.
- Rubin CT, Lanyon LE. Regulation of bone formation by applied dynamic loads. J Bone Joint Surg [Am]. 1984;66(3):397-402.
- Rubin C, Turner S, Muller R, et al. Quantity and quality of trabecular bone in the femur are enhanced by a strongly anabolic, noninvasive mechanical intervention. J Bone Miner Res. 2002;17(2):349-357.
- Rubin C, Judex S, Qin Y. Low-level mechanical signals and their potential as a non-pharmacological intervention for osteoporosis. Age Ageing. 2006; 35-S2: ii32–ii36 doi:10.1093/ageing/afl082.
- Darendeliler MA, Zea A, Shen G, Zoellner H. Effects of pulsed electromagnetic field vibration on tooth movement induced by magnetic and mechanical forces: a preliminary study. Aust Dent J. 2007;52(4):282-287.
- Nishimura M, Chiba M, Ohashi T, et al. Periodontal tissue activation by vibration: intermittent stimulation by resonance vibration accelerates experimental tooth movement in rats. Am J Orthod Dentofacial Orthop. 2008;133:572-583.
Keller
- Uribe F, Padala S, Allareddy V, Nanda R. Patients’, parents’, and orthodontists’ perceptions of the need for and costs of additional procedures to reduce treatment time. Am J Orthod Dentofacial Orthop. 2014; 145:S65-73.
- Fletcher Spaght, 2013, Orthodontic Market Research Survey