Recognizing how technology has evolved the consumer experience in nearly every aspect of daily life, I’m continually assessing orthodontic innovations that can help me exceed patient expectations. It’s not enough for orthodontists to simply offer patients the latest orthodontic advancements, we must also be confident that the technology will help deliver quality results. That’s why I’ve been an Invisalign® (Align Technology Inc) provider for almost 15 years, but have only offered aligner therapy as my top choice to every patient for the past 3 years. I initially only offered aligner therapy for simple, straightforward cases because it was difficult to get teeth to track in the aligners and I often wasn’t pleased with the final result, even after several refinements. Motivation and compliance were also issues with longer treatment.
As industry trends show that braces patients still account for the overwhelming majority of the 2.8 million annual orthodontic case starts, my perception is that there still are orthodontists who are not confident they can achieve quality results when treating difficult cases with aligners.
The game-changer for me was AcceleDent® (OrthoAccel Technologies Inc), an FDA-cleared vibratory orthodontic device that is clinically proven to speed up treatment by as much as 50% and reduce discomfort. Having all my patients use AcceleDent practically guarantees all the control I want and need to achieve the treatment outcomes that I promise patients will actually happen. I’ve completed nearly 1,000 AcceleDent cases, giving me the confidence that with this innovative device, I can more predictably achieve an outcome for a patient than has previously been possible in orthodontics.
To demonstrate how I have been able to achieve unprecedented precision with my accelerated aligner therapy cases, I’ve compared four sets of “tooth twins.” These “tooth twins” compare patients who present with similar diagnoses, but were treated with different mechanics. When incorporating AcceleDent into treatment, I’m able to achieve superior outcomes for complex cases than with standard braces or aligner cases. Prior to seeing how AcceleDent enhances precision and predictability, I would have only treated many of these cases with braces.
These cases detail specific protocols to follow when using accelerated aligner therapy. Unless otherwise noted, my protocol is for aligner patients to change their trays every 7 days.
[metaslider id=29295]
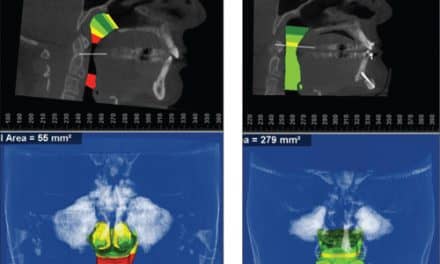
Tooth Twins: Class II—Distalization
Patient 1 and Patient 2 presented with a similar diagnosis: Class II malocclusions, prognathic maxilla, and severe overjet (Figure 1). Both male patients were adolescents at the time of treatment.
Patient 1 was treated several years ago, prior to my adoption of AcceleDent as standard of care; thus, I treated him with braces and a Pendex because I do not use headgear in my practice. Specifically, I used a Pendex appliance with Class II elastics off of a lower lingual holding arch to counteract the negative forces of protrusion on the maxillary anteriors. This patient completed treatment in 30 months (Figure 2).
Patient 2 was treated with Invisalign and AcceleDent. When approaching the distalization in this type of case with aligners, I find that you need to create the spaces first and then distalize into those spaces in order to retract anterior teeth and eliminate overjet. This is the precision in tooth movement I achieve with my accelerated aligner patients. If tooth movement during treatment is not identical to the cartoon-like animation in ClinCheck®, the aligner trays will stop fitting. If we’re not getting the exact amount of distalization that’s predicted, there will be more plastic between the teeth in the trays than in the mouth and the trays will not fit.
Specifically for Patient 2, I distalized U67s first to create a large space between the U6 and U5. Then I distalized the U45s creating distal spaces to both U3s. Finally I retracted U3-3.
Patient 2 completed accelerated aligner therapy in 9.75 months with 36 aligners (Figure 2). His estimated treatment length was 18 months. A significant component of achieving the predicted result was the patient’s compliance with AcceleDent, Invisalign, and the Class II elastics. Initially in reviewing his x-ray, I thought distalization might impact his maxillary third molars, but his final x-ray shows virtually no change.
I have also successfully followed this same treatment approach with adult patients.
[metaslider id=29754]
Tooth Twins: Blocked-Out Canines
Patient 3 and Patient 4 presented with blocked-out canines (Figure 3). The difference in these two cases is that Patient 4, a male adolescent, was slightly more complex since he had maxillary midline deviation to the right and mandibular to the left. His crowding was also more significant. Both were treated with Invisalign.
The female adult, Patient 3, completed standard treatment in 37 months with 49 total aligners (Figure 4). I experienced quite a bit of difficulty throughout her treatment because the teeth were not tracking with the movements planned in virtual animation. Her crowding and crossbite correction also presented challenges throughout treatment. Of her 49 aligners, nearly half (26) were refinement trays. This is a case today that I would only treat using accelerated aligner therapy because I can achieve a better-quality finish, as is evident when compared to Patient 4.
Patient 4 received the accelerated aligner therapy with AcceleDent and Invisalign. I did not distalize because his maxillary second molars were not erupted and I did not want them to become impacted. The initial set of aligners only created an ideal midline situation to create space for the canine to erupt and alleviate crowding. I used auxiliaries to extrude the canine and create better interdigitation with the lower teeth. At the 6-month progress mark, I was satisfied with his Class I molar occlusion and decided that there was no need for distalization. We achieved optimal alignment with 25 aligners. Once his second molars erupted, he wore 12 refinement aligners without attachments so I could coordinate all of the molars and improve the canine relationship. With refinement, his total treatment length was 9 months compared to an estimated 17-month treatment length (Figure 4).
[metaslider id=29755]
Tooth Twins: Spacing
Patient 5 and Patient 6 presented as spacing cases (Figure 5).
A female adolescent, Patient 5 was treated with suresmile® (OraMetrix Inc) braces without AcceleDent. Virtual treatment planning and customization is critical so I use suresmile with every braces case because it gives me the digital treatment planning I need to achieve excellent outcomes.
In addition to the spacing, we also corrected her bimaxillary protrusion, edge-to-edge overbite, and edge-to-edge overjet. Her total treatment time was 12 months (Figure 6).
Patient 6, a female adult, had very similar spacing as Patient 5, but because she received the accelerated aligner therapy with AcceleDent, she completed treatment in 5 months with 26 aligners (Figure 6). AcceleDent provides a significant advantage when treating spacing cases with aligners because it helps the teeth track. If the teeth do not track 100% according to the ClinCheck, the aligner trays will not fit. My protocol is 7 to 10 days with each aligner depending on the severity of spacing. Before using AcceleDent, I was instructing patients with generalized spacing to wear each aligner for 3 weeks.
[metaslider id=29756]
Tooth Twins: Exposure/Extrusion
Patient 7 and Patient 8 presented with impacted canines on the buccal. Patient 7, a male adolescent, had another impacted canine on the palate, which had the typical surgical exposure.
Patient 7 was treated with braces and no AcceleDent. To treat the impacted canines on the buccal, we tied them to bring the canines into the arch (Figure 7). He completed treatment in 36 months.
A female teen, Patient 8, was treated with AcceleDent and Invisalign. To correct Patient 8’s impacted canines, we used a soft tissue laser and then we performed alveoloplasty to score the bone and expose the canines. A week after the exposure, we bonded plastic buttons on her aligner trays for the canines to give her more of a horizontal and vertical vector (Figure 8). The reason I chose horizontal in addition to vertical is because I needed to pull the canines out and then down so as not to run into the alveolar housing.
Within 3 months, the canines moved down as predicted. One month later, the canines were in near perfect occlusion. In my experience, when patients are not using AcceleDent, it typically takes canines at least 12 months to move into position from the time of exposure. Since the patient used AcceleDent, the teeth moved faster than the ClinCheck predicted, causing the aligner trays to actually stall her progress. My protocol to mitigate the slowed progression is to cut the canines out of the trays to let them erupt while monitoring her progress more frequently. Initially, the incisal edge of the canines was above the CEJ of the centrals. A month later, they were in perfect position, which allowed us to begin refinements. We did 10 refinement trays with attachments only on the maxillary canines to lock them into position so that they would not move back up.
When using AcceleDent for eruption/extrusion cases, it’s important to understand that there’s a race between the soft and hard tissue healing over the exposed tooth versus the tooth movement in the arch. As was the case with Patient 8, the teeth actually moved faster than what was planned in each aligner so you may need to section the trays to allow teeth to erupt without any restrictions.
Conclusion
When evaluating new technology for their practices, I believe the question orthodontists ask is: Will this allow me to provide the same or better outcomes to my patients? Specifically with aligners, the question for me was: Can I provide the same or better outcomes, regardless of how complex the case is, with aligner therapy as I can braces? My “tooth twin” cases demonstrate that the answer is consistently “yes” when integrating AcceleDent into treatment. OP
 Manal Ibrahim, DDS, is a diplomate of the American Board of Orthodontics and the owner of Innovative Orthodontic Centers in Illinois. She completed dental school at the University of Illinois and went on to obtain a certificate in Advanced Combined Prosthodontics. She practiced restorative, prosthetic, and implant dentistry for nearly 10 years before obtaining her Certificate in Orthodontics and Dentofacial Orthopedics at New York University. Due to this unique background, Ibrahim has the ability to treat orthodontic patients presenting with any degree of complexity.
Manal Ibrahim, DDS, is a diplomate of the American Board of Orthodontics and the owner of Innovative Orthodontic Centers in Illinois. She completed dental school at the University of Illinois and went on to obtain a certificate in Advanced Combined Prosthodontics. She practiced restorative, prosthetic, and implant dentistry for nearly 10 years before obtaining her Certificate in Orthodontics and Dentofacial Orthopedics at New York University. Due to this unique background, Ibrahim has the ability to treat orthodontic patients presenting with any degree of complexity.